
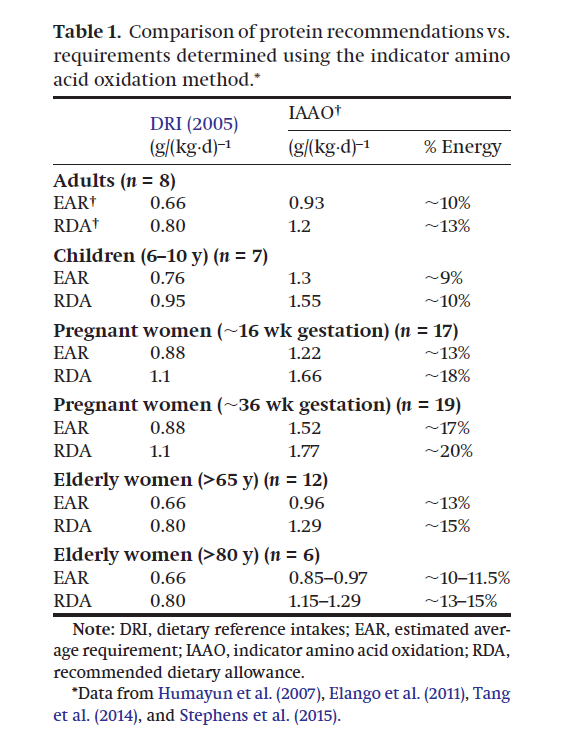
La question de l’apport optimal en protéines est très controversée. Les recommandations officielles conseillent habituellement un apport de l’ordre de 0,66g (EAR) ou 0,8g (RDA) par kilo de poids et par jour pour des personnes modérément actives, et jusqu’à 1,2g (RDA) pour des personnes très actives. Mais il est suggéré que cette recommandation serait une recommandation minimale qui ne prend pas en compte tous les besoins, et un certain nombre d’études d’observation semblent confirmer que l’apport optimal serait nettement supérieur. Ceci semble confirmé par une (relativement) nouvelle méthode d’estimation du besoin, l’IAAO, qui suggère un optimum environ 50% supérieur, s’étageant de 0,93g (EAR) ou 1,2g (RDA) pour des adultes modérément actifs à environ 2g (RDA), voire plus, pour les grands sportifs.
EAR : Estimate Average Requirement, besoin moyen estimé.
RDA : Recommanded dietary allowance, quantité recommandée (dose de sécurité permettant d’inclure l’essentiel de la population, les besoins étant variables selon les individus).
IAAO
Protein Requirements of Healthy Lactating Women Are Higher Than the Current Recommendations [PDF]
Rasmussen et al.
Current developments in nutrition, 2020
Our preliminary results suggest that the protein requirements for exclusively breastfeeding women (3–6 mo postpartum) is ∼1.7–1.9 g/kg/d.
Conclusions
Our findings for dietary protein needs during lactation are higher than the current EAR of 1.05 g/kg/d recommended by the DRI, suggesting that the recommendations may be underestimated. Our results correspond well with our earlier findings of higher protein needs of 1.52 g/kg/d during late stages of pregnancy (∼36 wk gestation) determined using the IAAO method.
–
Estimation of interindividual variability of protein requirement by indicator amino acid oxidation method [PDF]
Hayamizu et al.
Journal of clinical biochemistry and nutrition, 2020
From seven IAAO studies, the interindividual variability was estimated as a coefficient of variation of about 20%. The coefficient of variation of the protein requirement determined by IAAO study was wider than the ordinary coefficient of variation obtained from the nitrogen balance test.
–
Variable Intensity Exercise Increases Protein Requirements in Active Male and Female Adolescents as Determined by the Indicator Amino Acid Oxidation (IAAO) Technique [Abstract]
Jahmal C Brooks et al., 2017
The breakpoints derived herein exceed current estimated breakpoint values using the IAAO method for sedentary adults and children (0.93 g·kg−1·d−1, and 1.3 g·kg−1·d−1 respectively). Adjusting for the upper 95% CI, a recommended dietary allowance (RDA) was determined to be 1.83 g·kg−1·d−1 and 1.54 g·kg−1·d−1 for males and females respectively. Our estimate of the RDA in active adolescents exceeds the current protein RDA based on the factorial estimate of nitrogen balance for adolescents (0.9 g·kg−1·d−1)
–
Increased Protein Requirements in Female Athletes after Variable-Intensity Exercise [Abstract]
Wooding et al.
Medicine and science in sport and exercise, 2017
an estimated average requirement of 1.41 g·kg·d and recommended dietary allowance of 1.71 g·kg·d
–
Indicator Amino Acid–Derived Estimate of Dietary Protein Requirement for Male Bodybuilders on a Nontraining Day Is Several-Fold Greater than the Current Recommended Dietary Allowance [Texte] [PDF]
Bandegan et al.
The journal of nutrition, 2017
The Estimated Average Requirement (EAR) of protein and the upper 95% CI RDA for these young male bodybuilders were 1.7 and 2.2 g · kg−1 · d−1, respectively.
–
Protein Requirements Are Elevated in Endurance Athletes after Exercise as Determined by the Indicator Amino Acid Oxidation Method [Texte]
Kato et al.
Plos One, 2016
13CO2 excretion displayed a robust bi-phase linear relationship (R2 = 0.86) that resulted in an estimated average requirement and a recommended protein intake of 1.65 and 1.83 g protein·kg-1·d-1, respectively, which was similar to values based on phenylalanine oxidation (1.53 and 1.70 g·kg-1·d-1, respectively). We report a recommended protein intake that is greater than the RDA (0.8 g·kg-1·d-1) and current recommendations for endurance athletes (1.2–1.4 g·kg-1·d-1).
–
Recent developments in understanding protein needs – How much and what kind should we eat? [PDF]
Pencharz, Paul B. et al., 2016
Using IAAO we have shown that minimum protein requirements have been under estimated by 30-50%. The National Academy of Sciences have for macro-nutrients proposed “Acceptable Macronutrient Distribution Ranges”, which for protein is 10 to 35% of total energy. In practice, we suggest 1.5-2.2 g/kg/d of a variety of high-quality proteins.
–
Protein: A nutrient in focus [Texte]
Arentson-Lantz et al.
NRC research press, 2015
–
Amino Acid Metabolism and Protein Requirements in Active, Trained Adult Males Using the Indicator Amino Acid Oxidation (IAAO) Technique (thèse) [PDF]
JE. Packer
Université de Toronto, 2015
Accounting for a safe intake encompassing the upper 95%CI, the protein requirement of 1.64 g/kg/d determined herein exceeds the current dietary reference intake for non-active individuals as determined by NBAL (EAR = 0.66 g/kg/d; RDA = 0.80 g/kg/d) (FAO, WHO 2007) and the minimally invasive IAAO technique (EAR = 0.93 g/kg/d; RDA = 1.2 g/kg/d) (Humayun et al., 2007). In addition the minimum intake determined herein is at the upper range of general recommendations for athletes (i.e. 1.2-1.7g/kg/d) (American Dietetic Association et al., 2009).
–
Assessment of protein requirement in octogenarian women with use of the indicator amino acid oxidation technique [Page]
Tang et al.
The american journal of clinical nutrition, 2014
The mean protein requirement (95% CI) was 0.85 (0.60, 1.09) g · kg−1 · d−1. This requirement is 29% higher than the current Estimated Average Requirement (EAR) for adults of 0.66 g · kg−1 · d−1 based on the nitrogen balance technique, although the 95% CI includes the current EAR. The corresponding adequate protein allowance of 1.15 (0.77, 1.54) g · kg−1 · d−1 is 44% higher, although the 95% CI includes the Recommended Dietary Allowance (RDA) of 0.80 g · kg−1 · d−1.
–
Recent advances in determining protein and amino acid requirements
in humans [PDF]
Elango et al.
British journal of nutrition, 2012
The indicator amino acid oxidation (IAAO) method has emerged as a robust and minimally invasive technique to identify requirements. The IAAO method is based on the concept that when one indispensable dietary amino acid (IDAA) is deficient for protein synthesis, then the excess of all other IDAA, including the indicator amino acid, will be oxidized. With increasing intakes of the limiting amino acid, IAAO will decrease, reflecting increasing incorporation into protein. Once the requirement for the limiting amino acid is met there will be no further change in the indicator oxidation.
–
Protein requirement of healthy school-age children determined by the indicator amino acid oxidation method [Page]
Elango et al.
American journal of clinical nutrition, 2011
Mean and population-safe (upper 95% CI) protein requirements were determined to be 1.3 and 1.55 g · kg−1 · d−1, respectively. These results are significantly higher than the mean and population-safe protein requirements currently recommended by the DRI 2005 for macronutrients (0.76 and 0.95 g · kg−1 · d−1, respectively).
Etudes d’observation et avis
Optimizing Adult Protein Intake During Catabolic Health Conditions [Texte]
Phillips et al.
Advances in nutrition, 2020
Although the RDA for protein of 0.8 g/kg body weight is adequate to avoid obvious inadequacies, multiple studies provide evidence that many adults may benefit from protein quantity, quality, and distribution beyond guidelines currently defined by the RDA. Further, the dietary requirement for protein is a surrogate for the constituent amino acids and, in particular, the 9 considered to be indispensable. Leucine provides an important example of an essential amino acid where the RDA of 42 mg/kg body weight is significantly less than the 100–110 mg/kg required to optimize metabolic regulation and skeletal muscle protein synthesis. This review will highlight the benefits of higher protein diets to optimize health during aging, inactivity, bed rest, or metabolic dysfunction such as type 2 diabetes.

–
High Versus low Dietary Protein Intake and Bone Health in Older Adults: a Systematic Review and Meta-Analysis [Texte]
Groenendijk et al.
Computational and structural biotechnology journal, 2019
Meta-analysis of four cohort studies showed that higher protein intakes resulted in a significant decrease in hip fractures (pooled hazard ratio: 0.89; 95% confidence interval: 0.84, 0.94). This systematic review supports that a protein intake above the current RDA may reduce hip fracture risk and may play a beneficial role in BMD maintenance and loss in older adults.
–
Nutrition Recommendations for Bodybuilders in the Off-Season: A Narrative Review [PDF]
Iraki et al.
Sports, 2019
Sufficient protein (1.6–2.2 g/kg/day) should be consumed with optimal amounts 0.40–0.55 g/kg per meal and distributed evenly throughout the day (3–6 meals)
–
Perspective: Protein Requirements and Optimal Intakes in Aging: Are We Ready to Recommend More Than the Recommended Daily Allowance? [Texte]
Traylor et al.
Advances in nutrition, 2018
We propose that it should be recommended that older individuals consume ≥1.2 g protein · kg−1 · d−1 and that there should be an emphasis on the intake of the amino acid leucine, which plays a central role in stimulating skeletal muscle anabolism. Critically, the often-cited potential negative effects of consuming higher protein intakes on renal and bone health are without a scientific foundation in humans.
–
Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group [Texte]
Deutz et al.
Clinical nutrition, 2014
Based on the evidence presented and discussed, the following recommendations are made (a) for healthy older people, the diet should provide at least 1.0–1.2 g protein/kg body weight/day, (b) for older people who are malnourished or at risk of malnutrition because they have acute or chronic illness, the diet should provide 1.2–1.5 g protein/kg body weight/day, with even higher intake for individuals with severe illness or injury, and (c) daily physical activity or exercise (resistance training, aerobic exercise) should be undertaken by all older people, for as long as possible.
–
Dietary Guidelines should reflect new understandings about adult protein needs [Texte]
Donald K. Layman
Nutrition & metabolism, 2009
Protein is a critical part of the adult diet
Protein needs are proportional to body weight; NOT energy intake
Adult protein utilization is a function of intake at individual meals
Most adults benefit from protein intakes above the minimum RDA
[…] The developing controversy about Dietary Guidelines for protein stems from current perceptions that protein intakes above minimum requirements have no benefit and may pose long-term health risks. These beliefs are largely based on assumptions and extrapolations with little foundation in nutrition science. Diets with increased protein have now been shown to improve adult health with benefits for treatment or prevention of obesity, osteoporosis, type 2 diabetes, Metabolic Syndrome, heart disease, and sarcopenia [1–4]. This editorial argues that we need Dietary Guidelines that recognize these benefits and emphasize the right amounts of protein at specific meals.
[…] The new research establishes health benefits and provides molecular evidence of numerous metabolic outcomes associated with protein intake or amino acid metabolism that are not reflected in the traditional measure of nitrogen balance. These outcomes include cell signaling via leucine [7, 8], satiety [9, 10], thermogenesis [11], and glycemic control [12, 13]. The dietary protein necessary to optimize each of these metabolic outcomes is not reflected in measures of nitrogen balance and is not represented within the current concept of the minimum RDA.
–
Optimal protein intake in the elderly [PDF]
Wolfe et al.
Clinical nutrition, 2008
There is an evidence that the RDA for elderly may be greater than 0.8 g/kg/day. Evidence indicates that protein intake greater than the RDA can improve muscle mass, strength and function in elderly. In addition, other factors, including immune status, wound healing, blood pressure and bone health may be improved by increasing protein intake above the RDA. […] It appears that an intake of 1.5 g protein/kg/day, or about 15–20% of total caloric intake, is a reasonable target for elderly individuals wishing to optimize protein intake in terms of health and function.
–
Autres études
Dietary leucine requirement of older men and women is higher than current recommendations [PDF]
Szwiega et al.
American journal of clinical nutrition, 2020
The estimated leucine requirement of older adults is more than double the amount in current recommendations. These data suggest that leucine could be a limiting amino acid in the diet of older adults consuming the current RDA for protein and those consuming a plant-based diet. In view of the functional and structural role of leucine, especially its importance in muscle protein synthesis, current leucine recommendations of older adults should be revised.
–
Remarque : cette publication se base sur les recommandations classiques. Si les recommandations basées sur l’IAAO sont exactes, il conviendrait de porter la recommandation 40 à 50% plus haut que ce qui est indiqué ici.
Protein dietary reference intakes may be inadequate for vegetarians if low amounts of animal protein are consumed [Abstract]
Kniskern & Johnston
Nutrition, 2011
This research suggests that the protein DRI for vegetarians consuming less than the expected amounts of animal protein (45% to 50% of total protein) may need to be adjusted from 0.8 to about 1.0 g/kg to account for decreased protein bioavailability.
